During filler injections, injectors generally tend to pinch or pull the tissues with the non-dominant hand for the ease of the procedure.
This technique leads to a change in the anatomy of tissue layers whilst held.
The pinch technique also increases the tissue space for injections by moving the mobile tissue layers away from the fixed ones.
Risky areas
Common danger zones where risks are higher are in the temporal area and for nerve damage in the zygomatic arch area.
Pinch Anatomy
Medical illustrations or cadaver dissections generally show facial structures without changes in their anatomical structures. However, practitioners often pinch or pull the skin during patient assessment and treatment, particularly for PDO thread treatments, which changes its original appearance. This difference in the internal tissue through pinching or pulling is referred to as pinch anatomy.
Anatomy knowledge is essential for safe aesthetic procedures.
It is necessary in order to prevent blood vessel and nerve damage.
Knowledge of this “pinch anatomy” in the temple can be used to the injector’s advantage to avoid important arteries and to place filler in the correct plane.
The Pinch Technique

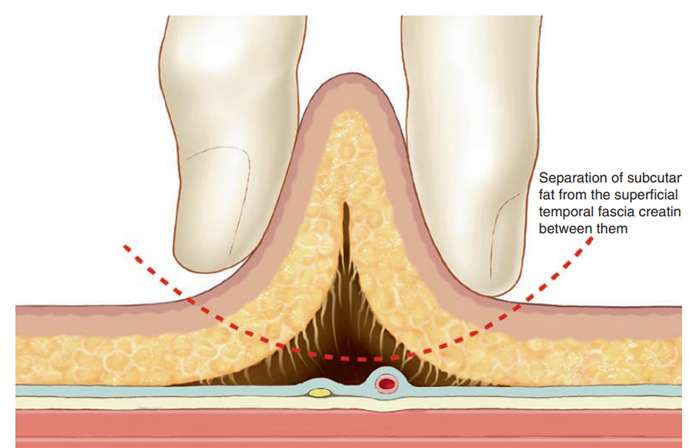
For extra safety we can carry out the pinch technique before an entry needle is inserted.
This helps the separation of the fat from the superficial fascia and helps us determine how much depth we have minimising the risk of vascular or nerve trauma.
Always use a gentle pinch.
When a pinch is done, a certain area of the temporal tissue loosens, and this area is pulled up. –
GENTLE PINCH -When the pinch is gently applied, the Interface between the subcutaneous fat and the superficial temporal fascia becomes loose, and the gap is created between them.
DEEPER PINCH – When the pinch is deeply applied, the superficial temporal fascia is separated from the deep temporal fascia.

When the gentle pinch is applied, the superficial temporal vessel encased by the superficial temporal fascia remains at the bottom, while subcutaneous fat is pulled upward with the skin. With the knowledge of pulled up layers with different pinch methods, practitioners can be more confident when carrying out treatment.
Zygomatic Arch Area
The facial nerve passes across the zygomatic arch. So, say when surgical facial lifting is per- formed, the facial nerve can be injured causing frontalis muscle weakness and eyebrows sagging. Also, in case of carrying out certain Aesthetic treatments, caution must be taken when the cannula is crossing the zygomatic arch or making an entry point with a needle in the area. The facial nerve runs beneath the superficial temporal fascia, and it does not get lifted with gentle pinching. Therefore, the cannula can cross the zygomatic arch without damaging the facial nerve if it is advanced in the subcutaneous fat layer. You can always feel for the zygomatic arch and try to stay above it or below it is depending what technique you have chosen.
Area where manipulation of pinching is useful
• Temple area inside the hairline
– Pinching may reduce the likelihood of Damaging the superficial temporal vessel.
– Pinching may help the cannula to proceed at an appropriate depth without damaging blood vessels.
• Zygomatic arch area – When gentle pinch is applied, the facial Nerve located deep to the SMAS is not Pulled upward.
Temple Area Inside the Hairline Pinch anatomy in the temporal area shows a few points.
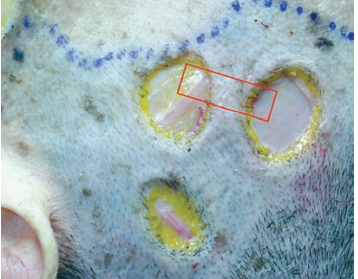
The result of cutting after pinching fat around the superficial temporal artery is removed almost completely. The fat layer located at the same depth as the blood vessel is damaged, while the blood vessel itself is intact.
When deep pinch was applied to the temporal area, the superficial temporal fascia was also removed along with the skin and subcutaneous fat.
Through cutting after pinching, the subcutaneous fat layer was removed, and the superficial temporal fascia was exposed. Damage to the superficial temporal fascia was not visible. Only the subcutaneous fat layer was presumed to be pulled upward by the pinch. This shows that the superficial temporal fascia was not pulled upward easily by a gentle pinch. Based on the lack of difference in the border of cut skin and the subcutaneous fat layer, it can be assumed that the pinch separated the subcutaneous fat layer from the fascia beneath. The superficial temporal artery is surrounded by the superficial temporal fascia, but it sticks out to the subcutaneous fat layer. The entire fat layer was removed without damage to the artery, which supports that the pinch caused separation of the subcutaneous fat layer and the superficial temporal fascia
The red square indicates the orientation of the tissue specimen. There is almost no subcutaneous fat layer in the temple area inside the hairline.
FAT LAYER REMOVED AT THE PINCH DEPTH
During the pinch technique, important arteries in that region get pulled up with the tissue layers held in a pinch or stay in their position unaffected.
When you pinch the tissues, the underlying blood vessels and nerves move with them. What layer of the skin and whether blood vessels and nerves are pulled upward during this process can determine if going deeper or more superficial would be the safer treatment method.
Knowing what anatomical changes occur through different methods of pinching can help minimize the risk of complications, such as blood vessel damage in the temporal area or nerve damage in the zygomatic arch area.
Leave a Reply